Utility of Biomarkers in Cardiac Amyloidosis
State-of-the-Art Review
Central Illustration

Abstract
Cardiac amyloidosis is a growing field, with advancements in diagnosis and management. Cardiac biomarkers are used to predict survival and to develop severity staging systems. Cardiac biomarkers are also used in clinical practice to stratify patients for treatment and to evaluate response to therapies. The current review summarizes the major clinical utility of current biomarkers in patients with cardiac amyloidosis and provides insights about future areas of investigation.
Highlights
| • | Biomarkers can be used for patients with light chain amyloidosis and transthyretin amyloidosis for staging and prognosis. | ||||
| • | Biomarkers can be used for patients with light chain amyloidosis to determine disease progression and response to therapies. | ||||
| • | The role of biomarkers to determine disease progression and response to therapies in patient with transthyretin amyloidosis is an active area of investigation. | ||||
Introduction
Amyloidosis refers to a group of systemic diseases caused by the extracellular accumulation of insoluble, misfolded protein aggregates in various organs (Figure 1) (1). The types of amyloidosis that are commonly associated with cardiac involvement are acquired monoclonal immunoglobin light chain amyloidosis (AL), wild-type transthyretin amyloidosis (ATTRwt), and hereditary transthyretin amyloidosis (ATTRm) (2). Regardless of cause, the degree of cardiac involvement at the time of diagnosis is the most important prognostic indicator.

Amyloidosis Fibril Deposition
A precursor protein misfold and an aggregate into amyloid fibrils. Amyloidosis fibrils deposit in the extracellular space of several organs. In the myocardium, it causes predominantly diastolic heart failure with release of biomarkers. BNP = brain natriuretic peptide; NT-proBNP = N-terminal pro–B-type natriuretic peptide.
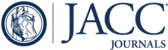
The purpose of this review was to summarize the history and current clinical use of cardiac biomarkers for assessment of prognosis and response to therapy in cardiac amyloidosis (Central Illustration) and to describe the ongoing areas of investigation into cardiac amyloidosis.

Utility of Biomarkers in Cardiac Amyloidosis
Cardiac biomarkers can be used to estimate staging and prognosis and also to assess response to therapies and disease progression. ATTR = transthyretin amyloidosis; cTnT/cTnI = cardiac troponin T/cardiac troponin I; eGFR = estimated glomerular filtration rate; NT-proBNP = N-terminal pro–B-type natriuretic peptide.
Cardiac Biomarkers for Staging and Prognosis
Staging of AL
Staging of AL
The prognosis of patients with AL is highly dependent on the extent of cardiac involvement at the time of diagnosis. Given that cardiac troponins T (cTnT) and I (cTnI) have been shown to be both sensitive and specific markers of cardiac injury (3), Dispernzieri et al. (4) reported that patients with detectable cTnT or cTnI at diagnosis of AL had a median observed survival (OS) of 6 to 8 months compared to a median OS of approximately 21 months in patients with undetectable troponin levels. At the same time, Palladini et al. (5) analyzed the expression of N-terminal pro–B-type natriuretic peptide (NT-proBNP) in patients newly diagnosed with AL and found a correlation between elevated NT-proBNP levels and both clinical cardiac involvement and decreased OS.
A staging system for AL amyloidosis was developed in 2004 by using patients with newly diagnosed AL seen at the Mayo Clinic between 1979 and 2000. This system, later termed the MAYO2004 staging system, defined patients as Stages I to III based on the absence of elevated cardiac biomarker (Stage I) versus the presence of a single elevated cardiac biomarker, cTnT/cTnI or NT-proBNP (Stage II) versus the elevation of both cardiac biomarkers (Stage III), with a median OS of approximately 27, 11, and 4 months, respectively (p < 0.0001) (6). For this staging system, the threshold values of cardiac biomarkers were set at the lower limit of detection for cTnT at <0.035 μg/l, detection of cTnI at <0.1 μg/l, and at the upper limit of normal for NT-proBNP at <332 ng/l (Table 1) (6). The MAYO2004 staging system was revised and expanded in 2012 (MAYO2012) to include a third independent prognostic indicator of OS, the clonal free light chain burden difference of ≥18 mg/dl. This allowed for Stages I to IV with a median OS of approximately 94, 40, 14, and 6 months, respectively (p < 0.001) (Figure 2A) (7). In the MAYO2012 staging system, the cutoff value for NT-proBNP was 1,800 pg/ml, and the cutoff for cTnT was ≥0.025 ng/ml (Table 1) (7). The MAYO2012 system can also be calculated using high-sensitivity cTnT, however a cutoff of 40 pg/ml is recommended (8).

Survival of Patients With Amyloidosis Based on Staging
(A) Survival in patients with light chain amyloidosis using the MAYO2010 staging system. Adapted with permission from Kumar et al. (7). (B) Survival in patient with light chain amyloidosis using the MAYO3b staging system. Reproduced with permission from Wechalekar et al. (9). (C) Survival in patients with wild-type transthyretin amyloidosis (ATTR) amyloidosis. Reproduced with permission from Grogan et al. (4). (D) Survival in patients with mutant ATTR amyloidosis. Reproduced with permission from Gillmore et al. (13).
| First Author (Year) (Ref. #) (Staging System) | Type | Biomarkers Cutoff Values | Staging | Prognosis Median OS |
|---|---|---|---|---|
| Dispenzieri et al. 2004 (6) (MAYO2004) | AL | NT-proBNP <332 ng/l | Stage I = NT-proBNP and cTn below | Stage I = 27 m |
| cTnT <0.035 μg/l | Stage II = NT-proBNP and cTn only 1 above | Stage II = 11 m | ||
| cTnI <0.1 μg/l | Stage III = NT-proBNP and cTn above | Stage III = 4 m | ||
| Kumar et al. 2012 (7) (MAYO2012) | AL | cTnT ≥0.025 ng/ml NT-proBNP ≥1,800 pg/ml FLC-diff ≥18 mg/dl | Stage I = all below cutoff | Stage I = 94 m |
| Stage II = 1 above | Stage II = 40 m | |||
| Stage III = 2 above | Stage III= 14 m | |||
| Stage IV = 3 above | Stage IV = 6 m | |||
| Wechalekar et al. 2013 (9) (MAYO3b) | AL | NT-proBNP >8,500 ng/l | Stage IIIb = NT-proBNP >8,500 ng/l | Stage IIIb = 5 m |
A few studies have gone on to analyze the prognostic value of the Mayo staging system in patients undergoing treatment for AL. Wechalekar et al. (9) evaluated the outcomes in response to chemotherapy in a large cohort of patients classified as Stage III by the original Mayo staging system. The investigators’ results, published in 2013, demonstrated a median OS of 7.1 months and identified an ultra-high risk population (MAYO3b) characterized by NT-proBNP concentrations of >8,500 ng/l and troponin-T >0.035 μg/l (Table 1), with an OS of only 5 months (Figure 2B) (9).
The staging systems in AL amyloidosis have been accepted for prognosis in clinical practice; however, further research is required in specific populations, such as patients with atrial fibrillation, who are known to have elevated natriuretic peptides. Also, the natriuretic peptides are cleared by the kidneys, and their levels are affected by the glomerular filtration rate. Palladini et al. (10) demonstrated that, in patients with AL amyloidosis with an estimated glomerular filtration rate (eGFR) of <15 ml/min/1.73 m2, NT-proBNP loses its prognostic value, whereas the B-type natriuretic peptide still predicts survival. A study in 1,224 patients by Dittirch et al. (11) from the Heidelberg Center, compared the performance of all AL staging systems in patients with atrial fibrillation and in patients with an eGFR <50. They found that MAYO2004, MAYO2012, and MAYO3b performance remained significant in patients with eGFR <50. However, the performance of all of them is reduced in patients with atrial fibrillation but less affected in patients assessed using the MAYO3b system. These findings favor the MAYO3b system in patients with eGFR <50 and in patients with atrial fibrillation.
Staging of ATTR
In 2016, Grogan et al. (12) reported a retrospective review of patients with ATTRwt between 1965 and 2013 to explore cTnT and NT-proBNP as predictors of survival. Based on their findings, a staging system was proposed that uses the same Stages I to III, defined in the Mayo staging system for AL, based on the presence or absence of elevation in cTnT and/or NT-proBNP. The ATTRwt staging system uses a cutoff point for cTnT of ≥0.05 ng/ml; however, the cutoff value for NT-proBNP determined to be prognostic in ATTRwt was significantly higher, at 3,000 pg/ml, than the cutoff point of 1,800 pg/ml used by the revised Mayo staging system for AL (Table 2). The present study found a median OS of 66, 40, and 20 months for Stages I, II, and III, respectively (Figure 2C) (12).
| First Author, Year (Ref. #) | Type | Biomarkers Cutoff Values | Staging | Prognosis Median OS |
|---|---|---|---|---|
| Grogan et al., 2016 (12) | ATTRwt | cTnT ≥0.05 ng/ml NT-proBNP ≥ 3,000 pg/ml | Stage I = all below cutoff | Stage I = 66 m |
| Stage II = 1 above | Stage II = 40 m | |||
| Stage III = 2 above | Stage III = 20 m | |||
| Gillmore et al., 2017 (13) | ATTRm | NT-proBNP ≥ 3,000 ng/l eGFR ≤ 45 ml/min | Stage I = NT-proBNP ≤3,000 ng/l and eGFR ≥45 ml/min | Stage I = 69 m |
| Stage II = all other combinations | Stage II = 47 m | |||
| Stage III = NT-proBNP >3,000 ng/l and eGFR <45 ml/min | Stage III = 24 m |
Until very recently, no formal staging system had been proposed for ATTRm cardiac amyloidosis. In 2017, Gillmore et al. (13) proposed a staging system based on NT-proBNP and eGFR that used retrospective analysis of a mixed population of patients with ATTR cardiac amyloidosis identified as having ATTRwt, p.Val142Ile (V122I) ATTRm or other ATTRm (13). Similar to the staging system proposed by Grogan et al. (12), the study by Gillmore found that the optimal cutoff point for NT-proBNP was 3,000 pg/ml and 45 ml/min/1.73 m2 for eGFR. It defines Stages I (NT-proBNP and eGFR less than or equal to the cutoff point) to III (both NT-proBNP and eGFR above the cutoff point) (Table 2), with OS of the combined cohort for Stages I, II, and III as approximately 62, 47, and 24 months, respectively (Figure 2D). Although this staging system is presented as being applicable to both ATTRwt and ATTRm, it was noted that on subgroup analysis, the V122I mutation seems to be associated with a shorter OS in all 3 stages; however, this mutation is predominant in some ethnic groups, and the shorter survival could result from multiple factors besides genotype (13).
Serum transthyretin (TTR), also known as prealbumin, is another biomarker that has been evaluated for prognosis. In a recent study by Hanson et al. (14), patients with ATTRwt with low serum levels of TTR <18 mg/dl (normal range, 18 to 45 mg/dl) had a median survival of 2.8 years, compared to 4.1 years in patients with serum TTR levels above the cutoff.
There are some considerations for the interpretation of cardiac troponins. Biomarker cTnI has several manufacturers and essays that are not harmonized, and the results are not comparable among the essays. In contrast, cTnT essays are developed from only 1 manufacturer and have good standardization, making results comparable among them. High-sensitivity troponin essays were introduced for earlier detection of myocardial injury; however, they require specific cutoff values based on sex, and healthy individuals can have small undetectable levels (15).
Cardiac Biomarkers for Assessment of Response to Therapy
Assessment of therapeutic response in AL
Assessment of therapeutic response in AL
The potential utility of NT-proBNP as a tool to assess response to therapy for patients with AL was alluded to in the first study by Palladini et al. (5), which showed that most patients with elevated NT-proBNP levels at diagnosis who achieved hematologic response to treatment also demonstrated a significant reduction in their NT-proBNP levels. Since that time, several studies of patients receiving treatment for AL have demonstrated a significant correlation between a defined decrease in NT-proBNP (NT-proBNP response) (16) and increased overall survival in response to therapy (17), confirming the utility of cardiac biomarkers in the assessment of response to treatment. The first of these studies, a prospective study published in 2006, demonstrated both clinical improvement in heart failure symptoms and prolonged median OS in patients who achieved both an NT-proBNP and a hematologic response following 3 cycles of chemotherapy, whereas patients who had progression of NT-proBNP levels did not receive clinical or survival benefits, despite a demonstrated hematologic response (18). These findings were confirmed in larger, retrospective studies published in 2010. One of those studies examined specifically NT-proBNP levels at 6 months in response to various treatment regimens (19), and another study aimed specifically at evaluating the efficacy of bortezomib in treatment of AL (20). Later, in response to the need for updated criteria to assess hematologic and cardiac response to the treatment of AL, a consensus paper described updated criteria to assess hematologic and cardiac response to treatment of AL amyloidosis (21). The criteria were based on data from European and U.S. centers and validated in the cohort studied by Palladini et al. (10). That study demonstrated that a 30% reduction in the NT-proBNP levels in response to treatment is the best indicator of cardiac response and strongly correlated to increase median OS. In addition, that report showed that echogenic evidence of cardiac response, defined as a 2-mm reduction in interventricular septal thickness in response to treatment, was not associated with a survival benefit and that increases in cTnT/I of >33% post-treatment are predictive of poorer outcomes (21). The findings of this study contributed significantly to the 2012 consensus guidelines for treatment of AL that were updated to include the use of cardiac biomarkers for quantification of cardiac response (NT-proBNP) or progression of cardiac involvement (NT-proBNP or cTnT/I) (Table 3) (16).
| Heart response |
| 1. NT-proBNP response (>30% and >300 ng/l decrease in patients with baseline NT-proBNP ≥650 ng/l) or |
| 2. NYHA functional class response (≥2 class decrease in subjects with baseline NYHA functional class III or IV) |
| Heart progression |
| 1. NT-proBNP progression (>30% and >300 ng/l increase∗) or |
| 2. cTn progression (≥33% increase), or |
| 3. Ejection fraction progression (≥10% decrease) |
Assessment of therapeutic response in ATTR
Several new therapies aimed at the reduction, stabilization, or degradation of TTR have emerged recently (22). Cardiac biomarkers, mainly NT-proBNP, along with imaging and clinical symptoms have been used in clinical trials in an effort to quantify the impact of a few of these new therapies on cardiac function.
TTR protein stabilizers, such as diflunisal, tafamidis, and AG-10, are medications directed at the stabilization of the TTR tetramer (2). Three small, single-arm clinical trials have searched for evidence of the efficacy of diflunisal, 250 mg twice daily, in ATTR cardiac amyloidosis using cardiac biomarkers. The first of those studies, published in 2012 (23) analyzed BNP and cTnI in 12 patients with ATTRwt or ATTRm at baseline and at 1 year. In that population, there was a small upward trend in both BNP and cTnI over the course of treatment without associated changes in cardiac structure or function (23). The results of the second study, published in 2015 (24), which monitored cardiac parameters, including BNP, in 28 Japanese patients with ATTRm over a minimum of 12 months, demonstrated nonsignificant fluctuations in BNP over the follow-up period and evidence of slow clinical deterioration in cardiac function over approximately 2 years (24). More promising are the results of the third study, published in 2018, which showed that, in 12 patients with ATTRwt treated with diflunisal, the levels of serum TTR were higher and the cTnI levels remained stable after 2 years of therapy compared to those in 23 untreated patients (14).
The efficacy of tafamidis, 20 mg once daily, in treating amyloid cardiomyopathy was assessed by using cardiac biomarkers in 2 small, single-arm clinic trials, both of which were published in 2015. The first of those studies (25) presented post hoc analysis of an open-label study that monitored cardiac parameters in 21 patients with ATTRm (excluding p.Val50Met [V30M] and V122I mutations). That study did not demonstrate any significant change in NT-proBNP over the course of 12 months of treatment in patients presenting with either elevated or normal NT-proBNP levels. cTnI remained stable over the course of the study (25). The second study (26) included both patients with ATTRwt and those with ATTRm with the V122I mutation. However, the results were only reported for the 31 patients with ATTRwt. There was a nonsignificant elevation in NT-proBNP and an average increase in cTnT/I in that population after 12 months of treatment with tafamidis. In the absence of a control group, biomarker results were compared to those reported for the patients with ATTRwt in the TRACS (Transthyretin Amyloidosis Cardiac Study) observational cohort (27), which had demonstrated a larger, increase in NT-proBNP over a similar time period and indicated that tafamidis was able to slow progression of cardiac disease (26). Recently, the results of the first phase III study of tafamidis (ATTR-ACT [Tafamidis in Transthyretin Cardiomyopathy Clinical Trial]) were published. The multicenter trial randomized 264 patients with ATTR amyloidosis (wild-type and mutant) to receive either 80 mg of tafamidis, 20 mg of tafamidis, or placebo in ratio of 2:1:2 for 30 months. Tafamidis demonstrated a significant reduction in all-cause mortality compared to placebo (29.5% vs. 42.9%) and a significant reduction of cardiovascular related hospitalizations (0.48 per year vs. 0.70 per year, respectively). These outcomes were calculated using aggregate data for the 2 doses and prespecified analysis of 80 versus 20 mg showed similar benefits. In relation to biomarkers, the study found that the patients who received tafamidis had lower elevations (least squares mean differences) in NT-proBNP than those who received placebo at months 12 (−735.14) and 30 (−2,180.54), suggesting a sustained biologic effect over time related to tafamidis (28).
AG-10 is a new TTR stabilizer that was tested in a phase II clinical trial in 49 patients with ATTR cardiomyopathy (wild type or mutant). Subjects were randomized to receive 400 mg or 800 mg or placebo in 1:1:1 ratio. Subjects taking AG10 achieved more than 90% stabilization of the tetrater with satisfactory safety and tolerability. The study measured serum TTR levels (pre-albumin) as a surrogate endpoint for in vivo response to therapy. At day 28, patients receiving 400 and 800 mg of AG-10 had higher levels of 36% and 50% TTR, respectively; but patients taking placebo experienced a reduction of 7% (29). Similar to the measurement of levels of diflunisal (14), serum levels of TTR have the potential to become a cost-effective method to assess response to therapy in patients with ATTR amyloidosis (30).
Amyloid degraders, such as the combination therapy of doxycycline and secondary bile acids are hypothesized to act synergistically to reduce deposition of TTR and degrade the TTR amyloid matrix already deposited in tissues. The first clinical trial to assess the efficacy of this class of therapy on ATTR cardiac amyloidosis was a small, phase II, open-label study using doxycycline and tauroursodeoxycholic acid (TUDCA) (31). Only 7 patients completed the full 12 months, and all of those patients had evidence of cardiac involvement at baseline. NT-proBNP levels increased in 3 patients and remained stable in 4, and no patients exhibited clinical evidence of cardiac progression (31). Another phase II study (32) published in 2017 evaluated the combination of doxycycline and ursodeoxycholic acid (UDCA) in patients with known ATTR cardiac amyloidosis; however, in that study, doxycycline was intermittently discontinued for periods of 2 weeks after every 4 weeks of treatment. Only 14% of the initial 28 patients completed the study. NT-proBNP levels remained stable for the first 6 months but rose significantly at 1 year. Participation in the study was terminated early for 14% of patients due to treatment failure, which was defined as a 30% increase in NT-proBNP from baseline (32).
Recent publications with TTR gene silencers have provided encouraging results for cardiac response to therapy. The APOLLO study, published in 2018, randomized 225 patients with ATTRm and polyneuropathy to patisiran therapy, 0.3 mg/kg or placebo once every 3 weeks. That study demonstrated a significant improvement in neuropathy and quality of life; and in a subgroup of patients with cardiac involvement, there was a decrease in the NT-proBNP-to-baseline ratio of 0.89 in the patisiran arm at 18 months compared to 1.89 in the placebo group, suggesting improved cardiac function (33). A subsequent publication focused on the outcomes in 126 patients with cardiac involvement defined as patients with left ventricular wall thickness ≥13 mm and no history of aortic valve disease or hypertension. In that cardiac population, patients taking patisiran had a 55% reduction in NT-proBNP at 18 months compared to placebo (a fold-change patisiran-to-placebo ratio of 0.45; 95% confidence interval: 0.34 to 0.59; p = 7.7 × 10−8 (34).
Novel biomarkers in AL and ATTR
At least 10 other novel biomarkers have been studied in patients with cardiac amyloidosis (Table 4). Of the biomarkers evaluated, preliminary studies suggest that von Willebrand factor (35), mid-regional pro-adrenomedullin (36), growth differentiation factor-15 (37,38), osteopontin (39), soluble suppression of tumorigenicity 2 (40), and osteoprotegerin (41) may be able to improve prognostication in high-risk patients with AL cardiac amyloidosis when substituted for or used in conjunction with the existing Mayo staging systems. Preliminary studies also suggested that high-sensitivity cardiac troponin T (hs-cTnT) had the potential to improve the sensitivity of the Mayo staging system (19,42). Although the most recent study did not show that hs-cTnT was able to contribute additional prognostic information to the existing staging systems, it did demonstrate its potential to simplify the prognostic algorithm by replacing the combination of NT-proBNP and a cardiac troponin in the Mayo staging system (43). Additional areas of study in cardiac amyloidosis using novel biomarkers include the evaluation of matrix metalloproteinases and tissue inhibitors of metalloproteinases to differentiate between AL and ATTR cardiac amyloidosis (44,45) and the use of both hs-cTnT (46) and hepatocyte growth factor (47) to differentiate between cardiac amyloidosis and other causes of cardiomyopathy (38).
| First Author (Ref. #) | Year | Biomarker | Amyloid | Purpose or Clinical Implication |
|---|---|---|---|---|
| Dispenzieri et al. (4) | 2003 | cTnT/cTnI | AL | Evaluation of cTnT and cTnI as biochemical markers of cardiac dysfunction and utility as prognostic indicators. |
| Palladini et al. (5) | 2003 | NT-proBNP | AL | Evaluation of NT-proBNP as a biochemical marker of cardiac dysfunction and utility prognostic indicator. |
| Dispenzieri et al. (6) | 2004 | NT-proBNP, cTnT/cTnI | AL | Elevation of NT-proBNP and/or cTnT/cTnI in a prognostic staging system (Mayo staging system). |
| Dispenzieri et al. (48) | 2004 | NT-proBNP, cTnT/cTnI | AL | Application of Mayo staging system with NT-proBNP and cTnT/cTnI to patients undergoing PBSCT. |
| Palladini et al. (18) | 2006 | NT-proBNP | AL | Evaluation of NT-proBNP as an indicator of response to chemotherapy in patients with AL. |
| Biolo et al. (44) | 2008 | MMPs, TIMPs, BNP | AL and ATTR | Differential increase in MMP-9 and TIMP-1 in AL vs. ATTR CA suggesting underlying difference in cardiac ECM disruption. BNP elevation greater in AL CA. |
| Palladini et al. (19) | 2010 | NT-proBNP, hs-cTnT | AL | NT-proBNP predictive of response to treatment of cardiac AL. Potential increased accuracy in prediction of OS with use of hs-cTnT. |
| Kastritis et al. (20) | 2010 | NT-proBNP | AL | NT-proBNP response associated with improved outcomes in patients with AL treated with bortezomib. |
| Kristen et al. (42) | 2010 | hs-cTnT, NT-proBNP, cTnT | AL | Suggests that hs-cTnT could be very sensitive to the presence of cardiac amyloidosis. |
| Palladini et al. (36) | 2011 | MR-proADM, NT-proBNP, cTnI | AL | MR-proADM was shown to be superior to NT-proBNP as a predictor of early death using the Mayo staging system. |
| Kumar et al. (7) | 2012 | NT-proBNP, cTnT/cTnI | AL | Revised Mayo staging system using a higher cutoff for NT-proBNP and prior threshold for cTnT/cTnI. |
| Palladini et al. (21) | 2012 | NT-proBNP, cTnT/cTnI | AL | NT-proBNP response identified as main criteria for defining cardiac response to treatment. Elevation in cTnT/I post-treatment indicative of poorer outcome. |
| Ruberg et al. (27) | 2012 | NT-proBNP | ATTR | NT-proBNP levels increased in association with progression of ATTR (wt and V122I mutation) CA. –TRACS |
| Castano et al. (23) | 2012 | BNP, cTnI | ATTR | Evaluation of baseline and follow-up BNP and cTnI for evidence of cardiac response to treatment with diflunisal. |
| Obici et al. (31) | 2012 | NT-proBNP | ATTR | Evaluation baseline and follow-up NT-proBNP in response to treatment with doxy/TUDCA. |
| Pinney et al. (51) | 2013 | NT-proBNP, cTnT | ATTR | Found that elevation in cTnT and, to a lesser degree, NT-proBNP was associated with reduced OS in ATTRwt CA. |
| Wechalekar et al. (9) | 2013 | NT-proBNP, cTnT/cTnI | AL | Response to chemotherapy in patients with Mayo Stage III disease. NT-proBNP > 8,500 pg/ml is a poor prognostic indicator. |
| Tanaka et al. (45) | 2013 | MMPs, TIMPs, BNP, cTnI | AL and ATTR | The combination of MMP-2/TIMP-2, cTnI and BNP were highly discriminative for differentiating between AL and ATTR CA. Elevated levels of MMP-2 and TIMP-1, but not MMP-9 and TIMP-2 in AL CA. |
| Dispenzieri et al. (43) | 2014 | hs-cTnT, NT-proBNP, cTnT | AL | Hs-cTnT in place of cTn may simplify the prognostic algorithm by eliminating the need for NT-proBNP in Mayo staging. |
| Kristen et al. (50) | 2014 | MR-proANP, NT-proBNP | AL | Demonstrated that MR-proANP performs equivalently to NT-proBNP in the Mayo staging system. |
| Kastritis et al. (37) | 2014 | GDF-15, NT-proBNP, hs-cTnT | AL | Findings suggest that GDF-15 levels in Q4 were discriminative in high-risk patients, identifying a sub-set with a median OS of 3 months. |
| Kristen et al. (39) | 2014 | OPN, NT-proBNP, cTnT | AL | Elevated OPN associated with poorer outcomes; may discriminate better between high-risk patients when used with cTnT in the place of NT-proBNP. |
| Kastritis et al. (52) | 2015 | NT-proBNP, cTnT/cTnI | AL | NT-proBNP response post-treatment correlated to increased OS. Mayo staging system and elevated NT-proBNP level pre-treatment used to successfully risk-adapt the treatment regimen for increased 1-year OS in high-risk patients. |
| Sekijima et al. (24) | 2015 | BNP | ATTR | Evaluations of BNP at baseline and over a 1 to 2 yr follow-up-period in patients treated with diflunisal. |
| Damy et al. (25) | 2015 | NT-proBNP, cTnI | ATTR | Evaluation of NT-proBNP and cTnI in ATTRm (non-V30M or V122I mutations) treated with tafamidis. |
| Maurer et al. (26) | 2015 | NT-proBNP, cTnT/cTnI | ATTR | Evaluation of NT-proBNP and cTnT/I in patients with ATTRwt and known cardiac disease treated with tafamidis. |
| Dispenzieri et al. (40) | 2015 | sST2, Gal-3, NT-proBNP, cTnT | AL | Findings showed sST2 demonstrated independent prognostic value on multivariate modeling and may add additional prognostic information to biomarker staging systems. |
| Kastritis et al. (41) | 2015 | OPG, NT-proBNP | AL | Elevation of OPG was correlated to NT-proBNP elevation and demonstrated prognostic value independent of Mayo Stage. Q4 elevations associated with median 1 yr. OS. |
| Gertz et al. (49) | 2016 | NT-proBNP | AL | Demonstrated NT-proBNP response as evidence of cardiac response to treatment with NEOD001 an anti-LC antibody. |
| Connors et al. (53) | 2016 | BNP, cTnI | ATTR | BNP demonstrated prognostic significance in ATTRwt CA, cTnI did not show significant correlation. |
| Damy et al. (54) | 2016 | NT-proBNP, cTnT, hs-cTnT | AL and ATTR | NT-proBNP was a strong prognostic indicator in CA due to AL or ATTR. cTnT/hs-cTnT was only prognostic in AL. |
| Grogan et al. (12) | 2016 | NT-proBNP, cTnT | ATTR | Defines staging system for ATTRwt based on the Mayo staging system for AL. |
| Perfetto et al. (55) | 2016 | NT-proBNP | AL and ATTR | Comparison of NT-proBNP levels in AL, ATTRwt, and ATTRm CA with similar findings on ECHO. Identifies notable differences in NT-proBNP between all 3 types of CA. |
| Kristopher et al. (47) | 2016 | HGF, Gal-3 | AL and ATTR | Study looking to differentiate CA from systemic AL or other cardiomyopathies. HGF elevation associated with both AL and ATTR CA, however also elevated in HFrEF. Gal-3 only elevated in systemic AL, not AL CA. |
| Kastritis et al. (35) | 2016 | VWF, ADAMTS-13 | AL | High VWF levels demonstrated prognostic significance. |
| Wixner et al. (32) | 2017 | NT-proBNP | ATTR | Evaluation of NT-proBNP in patients with ATTR CA at baseline and during treatment with doxy/UDCA. |
| Kristen et al. (56) | 2017 | NT-proBNP, cTnT/cTnI | ATTR | Demonstrates that Q4 elevations of NT-proBNP, cTnT and cTnI are independent predictors of survival in ATTR. |
| Siepen et al. (57) | 2017 | NT-proBNP | ATTR | Identified NT-proBNP as an independent predictor of mortality in ATTRwt CA. |
| Takashio et al. (46) | 2017 | hs-cTnT, BNP | AL and ATTR | Found hs-CTnT levels to be significantly higher in CA compared to other causes of cardiac hypertrophy |
| Gillmore et al. (13) | 2017 | NT-proBNP | ATTR | Defines staging system based on NT-proBNP and eGFR applicable to ATTRwt and ATTRm |
| Hanson et al. (14) | 2018 | Serum TTR, cTnI | ATTR | Serum TTR levels for prognosis and response to therapy |
| Kastritis et al. (66) | 2018 | GDF-15 | AL | GDF-15 predicts mortality, progression to dialysis, and response to therapy |
| Adams et al. (33) | 2018 | NT-proBNP | ATTR | Clinical trial of patisiran in patients with ATTRm and neuropathy |
| Judge et al. (29) | 2019 | Serum TTR | ATTR | Serum TTR levels for in vivo response to therapy |
Conclusion and Future Prospects
In AL cardiac amyloidosis, cardiac biomarkers have been used successfully to develop staging systems that have been consistently validated in predicting baseline prognosis at time of diagnosis and have demonstrated utility in predicting prognosis in response to treatment (6,7,48). In addition, NT-proBNP has been successfully established and validated as a surrogate marker for survival in AL based on treatment response (21,49). As advances in disease-modifying therapies continue to be developed and as ATTR cardiac amyloidosis has become an increasingly recognized cause of diastolic dysfunction in our aging population, the need for methods of early accurate diagnosis, risk stratification, and assessment of therapeutic response for cardiac amyloidosis will continue to grow. Cardiac biomarkers provide a noninvasive, easily accessible, relatively inexpensive method for evaluating cardiac disease and its progression, and have the potential to take on a more expansive role in the diagnosis and ongoing assessment of cardiac amyloidosis.
Review of how cardiac biomarkers have been used and studied in patients with cardiac amyloidosis reveals the need for continued investigation in a number of areas. Further risk stratification of patients with high-risk (Mayo Stages 3b and IV) AL cardiac amyloidosis is needed to direct and, if necessary, risk-adapt prompt therapeutic interventions. The addition of a higher NT-proBNP threshold or the use of a novel cardiac biomarker to further refine the Mayo staging system has been explored (19,36,37,39,41–43,50). Furthermore, the effects of atrial fibrillation and renal failure in the Mayo staging system require further investigation. Additionally, new treatment options for ATTR underscore the need for further evaluation of how cardiac biomarkers reflect prognosis and disease progression in ATTRwt and ATTRm cardiac amyloidosis to determine whether these biomarkers are accurate indicators of treatment response. Further delineation of how the natural history and the differences between ATTRwt and ATTRm are defined by cardiac biomarkers is necessary to better understand the implication of post-treatment cardiac biomarker levels (23–26,31,32). Finally, the recognition of ATTR cardiac amyloidosis as an underdiagnosed, treatable cause of diastolic heart failure, the significant difference in treatment of AL and ATTR, and the rapidly progressive nature of AL cardiac amyloidosis identify the need for simple, noninvasive methods of differentiating AL and ATTR cardiac amyloidosis from each other and from other causes of diastolic heart failure (44–46). As the diagnosis and treatment of cardiac amyloidosis continue to evolve rapidly, the use of cardiac biomarkers in this progressive, fatal disease process remains an exciting, clinically relevant area of active investigation.
Abbreviations and Acronyms
| ADAMTS-13 | metalloproteinase with thrombospondin type-1 repeats 13 |
| AL | light chain amyloidosis |
| ATTR | transthyretin amyloidosis |
| ATTRm | mutant transthyretin amyloidosis |
| ATTRwt | wild-type transthyretin amyloidosis |
| BNP | B-type natriuretic peptide |
| CA | cardiac amyloidosis |
| cTn | cardiac troponin |
| cTnI | cardiac troponin I |
| cTnT | cardiac troponin T |
| ECM | extra cellular matrix |
| eGFR | estimated glomerular filtration rate |
| Gal-3 | galactin-3 |
| GDF | growth differentiation factor |
| HFrEF | heart failure with reduced ejection fraction |
| HGF | hepatocyte growth factor |
| hs-cTn | high-sensitivity cardiac troponin |
| MMPs | matrix metalloproteinases |
| MR-proADM | mid-regional pro-adrenomedullin |
| MR-proANP | midregional pro-atrial natriuretic peptide |
| NT-proBNP | N-terminal pro–B-type natriuretic peptide |
| NYHA | New York Heart Association |
| OPG | osteoprotegerin |
| OPN | osteopontin |
| PBSCT | peripheral blood stem cell transplant |
| sST2 | soluble suppression of tumorigenicity 2 |
| TIMPs | tissue inhibitors of metalloproteinases |
| TUDCA | tauroursodeoxycholic acid |
| UDCA | ursodeoxycholic acid |
| VWF | von Willebrand factor |
References
1. "Molecular mechanisms of amyloidosis". N Engl J Med 2003;349:583-596.
2. "Cardiac amyloidosis: where are we today?"J Intern Med 2015;278:126-144.
3. "It's time for a change to a troponin standard". Circulation 2000;102:1216-1220.
4. "Survival in patients with primary systemic amyloidosis and raised serum cardiac troponins". Lancet 2003;361:1787-1789.
5. "Serum N-terminal pro-brain natriuretic peptide is a sensitive marker of myocardial dysfunction in AL amyloidosis". Circulation 2003;107:2440-2445.
6. "Serum cardiac troponins and N-terminal pro-brain natriuretic peptide: a staging system for primary systemic amyloidosis". J Clin Oncol 2004;22:3751-3757.
7. "Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements". J Clin Oncol 2012;30:989-995.
8. "Validation of Mayo Clinic staging system for light chain amyloidosis with high-sensitivity troponin". J Clin Oncol 2019;37:171-173.
9. "A European collaborative study of treatment outcomes in 346 patients with cardiac stage III AL amyloidosis". Blood 2013;121:3420-3427.
10. "Best use of cardiac biomarkers in patients with AL amyloidosis and renal failure". Am J Hematol 2012;87:465-471.
11. "Performance analysis of AL amyloidosis cardiac biomarker staging systems with special focus on renal failure and atrial arrhythmia". Haematologica 2019;104:1451-1459.
12. "Natural history of wild–type transthyretin cardiac amyloidosis and risk stratification using a novel staging system". J Am Coll Cardiol 2016;68:1014-1020.
13. "A new staging system for cardiac transthyretin amyloidosis". Eur Heart J 2017;39:2799-2806.
14. "Use of serum transthyretin as a prognostic indicator and predictor of outcome in cardiac amyloid disease associated with wild-type transthyretin". Circ Heart Fail 2018;11:e004000.
15. "Determination of 19 cardiac troponin I and T assay 99th percentile values from a common presumably healthy population". Clin Chem 2012;58:1574-1581.
16. "Consensus guidelines for the conduct and reporting of clinical trials in systemic light-chain amyloidosis". Leukemia 2012;26:2317-2325.
17. "Rationale, application and clinical qualification for NT-proBNP as a surrogate end point in pivotal clinical trials in patients with AL amyloidosis". Leukemia 2016;30:1979-1986.
18. "Circulating amyloidogenic free light chains and serum N-terminal natriuretic peptide type B decrease simultaneously in association with improvement of survival in AL". Blood 2006;107:3854-3858.
19. "The combination of high-sensitivity cardiac troponin T (hs-cTnT) at presentation and changes in N-terminal natriuretic peptide type B (NT-proBNP) after chemotherapy best predicts survival in AL amyloidosis". Blood 2010;116:3426-3430.
20. "Bortezomib with or without dexamethasone in primary systemic (light chain) amyloidosis". J Clin Oncol 2010;28:1031-1037.
21. "New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes". J Clin Oncol 2012;30:4541-4549.
22. "The transthyretin amyloidoses: advances in therapy". Postgrad Med J 2015;91:439-448.
23. "Diflunisal for ATTR cardiac amyloidosis". Congest Heart Fail 2012;18:315-319.
24. "Safety and efficacy of long–term diflunisal administration in hereditary transthyretin (ATTR) amyloidosis". Amyloid 2015;22:79-83.
25. "Cardiac findings and events observed in an open-label clinical trial of tafamidis in patients with non-Val30Met and non-Val122Ile hereditary transthyretin amyloidosis". J Cardiovasc Transl Res 2015;8:117-127.
26. "Tafamidis in transthyretin amyloid cardiomyopathy: effects on transthyretin stabilization and clinical outcomes". Circ Heart Fail 2015;8:519-526.
27. "Prospective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the Transthyretin Amyloidosis Cardiac Study (TRACS)". Am Heart J 2012;164:222-228.
28. "Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy". N Engl J Med 2018;379:1007-1016.
29. "Transthyretin stabilization by AG10 in symptomatic transthyretin amyloid cardiomyopathy". J Am Coll Cardiol 2019;74:285-295.
30. "Serum transthyretin: predictor of amyloidosis outcomes?"Circ Heart Fail 2018;11:e004802.
31. "Doxycycline plus tauroursodeoxycholic acid for transthyretin amyloidosis: a phase II study". Amyloid 2012;19:Suppl 1: 34-36.
32. "Effect of doxycycline and ursodeoxycholic acid on transthyretin amyloidosis". Amyloid 2017;24:78-79.
33. "Patisiran, an RNAi therapeutic, for hereditary transthyretin amyloidosis". N Engl J Med 2018;379:11-21.
34. "Effects of patisiran, an RNA interference therapeutic, on cardiac parameters in patients with hereditary transthyretin-mediated amyloidosis: an analysis of the APOLLO study". Circulation 2018;139:431-443.
35. "Clinical and prognostic significance of serum levels of von Willebrand factor and ADAMTS-13 antigens in AL amyloidosis". Blood 2016;128:405-409.
36. "Midregional proadrenomedullin (MR-proADM) is a powerful predictor of early death in AL amyloidosis". Amyloid 2011;18:216-221.
37. "Growth differentiation factor-15 in patients with light chain (AL) amyloidosis has independent prognostic significance and adds prognostic information related to risk of early death and renal outcomes". Blood 2014;124.
38. "Growth differentiation factor-15 is a new biomarker for survival and renal outcomes in light chain amyloidosis". Blood 2018;131:1568-1575.
39. "Osteopontin: a novel predictor of survival in patients with systemic light-chain amyloidosis". Amyloid 2014;21:202-210.
40. "Soluble suppression of tumorigenicity 2 (sST2), but not galactin-3, adds to prognostication in patients with systemic AL amyloidosis independent of NT-proBNP and troponin T". Am J Hematol 2015;90:524-528.
41. "Osteoprotegerin is a significant prognostic factor for overall survival in patients with primary systemic amyloidosis independent of the Mayo staging". Blood Cancer J 2015;5:e319.
42. "Assessment of disease severity and outcome in patients with systemic light-chain amyloidosis by the high-sensitivity troponin T assay". Blood 2010;116:2455-2461.
43. "High sensitivity cardiac troponin T in patients with immunoglobulin light chain amyloidosis". Heart 2014;100:383-388.
44. "Matrix metalloproteinases and their tissue inhibitors in cardiac amyloidosis: relationship to structural, functional myocardial changes and to light chain amyloid deposition". Circ Heart Fail 2008;1:249-257.
45. "Circulating matrix metalloproteinases and tissue inhibitors of metalloproteinases in cardiac amyloidosis". J Am Heart Assoc 2013;2:e005868.
46. "Diagnostic utility of cardiac troponin T level in patients with cardiac amyloidosis". ESC Heart Fail 2017;5:27-35.
47. "Plasma hepatocyte growth factor is a novel marker of AL cardiac amyloidosis". Amyloid 2016;23:242-248.
48. "Prognostication of survival using cardiac troponins and N-terminal pro-brain natriuretic peptide in patients with primary systemic amyloidosis undergoing peripheral blood stem cell transplantation". Blood 2004;104:1881-1887.
49. "Organ response in patients with AL amyloidosis treated with NEOD001, an amyloid–directed monoclonal antibody". Am J Hematol 2016;91:E506-E508.
50. "Evaluation of the clinical use of midregional pro-atrial natriuretic peptide (MR-proANP) in comparison to N-terminal pro-B-type natriuretic peptide (NT-proBNP) for risk stratification in patients with light-chain amyloidosis". Int J Cardiol 2014;176:1113-1115.
51. "Senile systemic amyloidosis: clinical features at presentation and outcome". J Am Heart Assoc 2013;2:e000098.
52. "Long-term outcomes of primary systemic light chain (AL) amyloidosis in patients treated upfront with bortezomib or lenalidomide and the importance of risk adapted strategies". Am J Hematol 2015;90:E60-E65.
53. "Heart failure resulting from age-related cardiac amyloid disease associated with wild-type transthyretin: a prospective, observational cohort study". Circulation 2016;133:282-290.
54. "Identification of prognostic markers in transthyretin and AL cardiac amyloidosis". Amyloid 2016;23:194-202.
55. "Different NT-proBNP circulating levels for different types of cardiac amyloidosis". J Cardiovasc Med 2016;17:810-817.
56. "Impact of genotype and phenotype on cardiac biomarkers in patients with transthyretin amyloidosis---report from the Transthyretin Amyloidosis Outcome Survey (THAOS)". PLoS One 2017;12:e0173086.
57. "Predictors of survival stratification in patients with wild-type cardiac amyloidosis". Clin Res Cardiol 2017;107:158-169.
Footnotes
Dr. Nativi-Nicolau’s institution has received funding for clinical trials from Pfizer, Akcea and Eidos; and educational grants from Pfizer; and he is a consultant for Pfizer, Eidos, Akcea, and Alnylam. Dr. Kovacsovics has received research support from Prothena and Janssen. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the JACC: Heart Failure author instructions page.
{kind=link}
{kind=link}
{kind=link}
{kind=link}