3D Printing and Heart Failure: The Present and the Future
State-of-the-Art Review
Central Illustration

Abstract
Advanced imaging modalities provide essential anatomic and spatial information in patients with complex heart disease. Two-dimensional imaging can be limited in the extent to which true 3-dimensional (3D) relationships are represented. The application of 3D printing technology has increased the creation of physical models that overcomes the limitations of a 2D screen. Many groups have reported the use of 3D printing for preprocedural planning in patients with different causes of heart failure. This paper reviews the innovative applications of this technique to provide patient-specific models to improve patient care.
Introduction
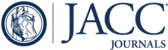
The origins of heart failure (HF) in both the pediatric and adult populations are numerous, complex, and multifactorial (1). Therapies for HF include medical, transcatheter, and surgical interventions. 3-dimensional (3D) printing technology is increasingly being used as an advanced imaging technique by which unique patient-specific models can be created for guidance prior to catheter-based or surgical interventions for patients with HF. This review highlights the role of 3D printing for preprocedural planning in patients with a wide variety of pathologies leading to HF (Central Illustration).

Causes of Heart Failure
(Left) 2D images of different causes of heart failure. (Right) Patient-specific 3D models created using a 3D printer.
3D Printing
Although 3D printing, also known as additive manufacturing or rapid prototyping, has been used in other industries for more than 30 years, medical 3D printing has become more common in the last 5 to 10 years. The exponential growth in its popularity has been associated mainly with the use of patient-specific physical models for pre-procedural planning. Advanced imaging techniques, such as cardiac magnetic resonance (CMR) or cardiac computed tomography (CCT), provide some of the anatomic detail needed to plan a complex procedure in patients with abnormal cardiac anatomy. Spatial visualization of the heart using these modalities, however, is limited in the sense that 3D renderings are displayed on a 2D screen. 3D printing is a technique that can offer additional anatomic information to aid in presurgical planning and decrease some of the potential difficulty associated with complete comprehension of 3D spatial relationships. The process of creating a 3D physical structure using a 3D printer involves first creating a virtual 3D object from a 3D image dataset through segmentation. This 3D file is then translated into a physical object using different techniques which vary depending on the type of printer used. The capabilities of printers vary widely in terms of the largest size model that can be printed (build volume), layer resolution, materials, and colors used for printing. Some printers have the ability to print in different colors within the same model, which can be useful, for example, when printing tumors within the myocardium (2). Other printers can print combinations of hard and soft materials, an ability that can help mimic tissue stiffness. This feature highlights the core advantage of using a physical 3D printed model compared to a virtual or digital model. The option of performing and practicing interventions using a physical model created in a pliable material offers a tangible experience impossible to recreate with a digital model. Specialties ranging from orthopedics to cardiology are applying 3D printing to create patient-specific models to aid in presurgical planning (3,4). 3D printing applications in pediatric patients with congenital heart disease (CHD) include visualizing intracardiac spatial anatomy before repair of double outlet right ventricles and tetralogy of Fallot with major aortopulmonary collateral arteries (5,6).
How Is a 3D Model Created?
A volumetric imaging dataset serves as the source for anatomical information to be converted to a 3D computerized and then physically printed model. This dataset may be obtained from CMR, CCT, echocardiography, or rotational angiography (7). Postprocessing of the imaging dataset involves identification of the region of interest and segmentation of this anatomy. Segmentation involves highlighting a particular part of the image dataset that will be included in the final model. A relatively simple left atrial segmentation is used to demonstrate the process (Figure 1). There are both commercial and open-source software programs available to perform this task. Mimics (Materialise, Leuven, Belgium), Seg3D (University of Utah, Salt Lake City, Utah), Slicer (8), Vitrea (Vital Images, Minnetonka, Minnesota), and Terarecon (Foster City, California) are examples of available software options. Segmentation can be a labor-intensive task, especially with a suboptimal dataset. Sharp blood pool-to-tissue contrast, fine spatial resolution (on the order of 1-mm isotropic for CMR or CCT), and lack of motion artifact characterize datasets that will be the easiest to post-process and produce the best 3D model. Given that the final model is a direct representation of the volumetric data, the model quality is only as good as the imaging from which it is derived. The area of interest that has been highlighted is then converted to computer-aided design format, which retains 3D spatial information and can be transformed into a physical object using a 3D printer. The surface of the 3D computerized model consists of a triangular mesh. Digital formats that are commonly used to store 3D files include STL, 3MF, VRML, PLY, OBJ, and AMF. Multi-material and multicolor prints require a 3D digital file to be stored in formats such as VRML, 3MF, and AMF, which can retain these characteristics.

Segmentation of a Cardiac CT to Create an LA Appendage Model
The orthogonal views of the left atrium are used to highlight the blood pool. Once the boundaries of the LA have been appropriately outlined, the software creates a 3D virtual model of the blood pool (bottom right). CT = computed tomography; LA = left atrium; LV = left ventricle; RV = right ventricle.
3D printers vary widely in their ability to create multicolor, multi-material models as well as achieve the highest resolution, build size, and print speed. Three common methods of 3D printing include fused deposition modeling, PolyJet (Stratasys, Eden Prairie, Minnesota), and stereolithography, and each has its own advantages. Fused deposition modeling (FDM) printers can use filaments made of any thermoplastic including poly-lactic acid (PLA) and acrylonitrile butadiene styrene (ABS) and can typically be found at a lower cost. The layer resolution of PolyJet and stereolithography printers tends to be finer than that of FDM, and PolyJet allows for multicolor and multi-material printing. Printer and material costs are factors that also come into play when choosing the best 3D printer for a specific program and purpose. Smaller desktop printers, such as the Mojo (Stratasys) and the Makerbot Replicator 2X (Makerbot, New York, New York) that print using FDM, can be acquired for a few thousand dollars, whereas industrial sized printers such as the J750 (Stratasys) and the ProX SLS 500 (3D Systems, Rock Hill, South Carolina) with advanced capabilities cost up to a few hundred thousand dollars. Once the 3D virtual file has been prepared for printing, it is processed by a 3D printer, and the task of creating a physical object one layer at a time begins. Any overhanging parts are typically printed with support material to maintain their position in space. Duration of the print depends largely on the size and complexity of the print and speed of the printer used. A life-sized adult cardiac model may take 24 h to print. The final 3D printed model is often encased in support material which is removed either manually or by soaking in a solution. Once the support material has been removed, the final 3D model is revealed (Figure 2).

Solid Model of the LA Blood Pool Is Hollowed
(A) Solid model of the LA blood pool is hollowed, allowing views of the intracardiac structure and saved as a 3D virtual file. (B) This STL file is then printed on a 3D printer and converted into a physical object. LAA = left atrial appendage; PV = pulmonary vein; STL = stereolithography; other abbreviations are as in Figure 1.
Practical considerations for implementing this technology at a medical center include costs involved with the post-processing software, printer, model material, and staff to perform the post-processing. Commercial software can cost upwards of $15,000 yearly for 1 license (e.g., Mimics, Materialise). Costs associated with the individual who performs the post-processing largely depends on whether a specialist, a physician, technologist, or engineer, is available on staff to perform this task at no extra cost. If not, an outside consultant may be hired to create the digital source model. Purchasing a printer that can create cardiac prints with reliable accuracy and detail fine enough to represent small vessels can be challenging for centers with limited resources. Those printers that create models with soluble supports offer the advantage of dissolving support material without damaging finer structures within the model (e.g., Mojo, Stratasys). This printer, refurbished, can be purchased for approximately $5,000. Aside from cost, an institution must ensure that the application of the 3D printed models in their hospital falls within U.S. Food and Drug Administration regulatory requirements (9). The decision to invest in 3D printing technology for procedural planning or teaching is multifactorial and varies by resources available and potential utility at a specific center.
Specific Applications for Treating Heart Failure
Transcatheter aortic valve replacement
Transcatheter aortic valve replacement
Fabrication of patient-specific models that replicate the flexibility of the left ventricular outflow tract and aortic root as well as rigid calcifications have allowed physiologic testing in models of aortic stenosis. Maragiannis et al. (10) demonstrated the feasibility of creating multi-material models from CCT–based image datasets which replicated the degree of aortic stenosis as confirmed by Doppler echocardiographic measurements when pulsatile flow loops were connected to the 3D printed outflows (Figure 3). The ability to create models with both the anatomic and physiologic properties of a specific patient allows optimization of a procedural plan prior to entering the operating room or catheterization laboratory. Paravalvular leaks are more common after transcatheter aortic valve replacement (TAVR) than surgical valve replacement and are associated with increased late mortality even when mild (11). Ripley et al. (12) retrospectively created models of the aortic root from CCTs in patients who had undergone TAVR in order to assess feasibility and to potentially predict cases in which there would be paravalvular leakage. Models were created for 16 patients, with excellent agreement of measurements of the aortic annulus between CCT and printed models. Six of nine patients with paravalvular leaks were correctly identified. Although a small cohort experienced leakage, and prediction of post-TAVR leakage was not perfect, this study demonstrates that 3D printed aortic roots may potentially be used along with other imaging modalities to choose patients who would be better suited for a TAVR with a potentially lower risk of paravalvular leaks (12). In an effort to identify a quantitative measurement by which paravalvular leaks may be predicted, Qian et al. (13) developed the maximum bulge index. Phantoms of the aortic root were 3D printed in a material mimicking the mechanical properties of biological tissue by using CCT source datasets (Figure 4). Strain distribution after TAVR implantation was evaluated using analysis of the change in position of small beads attached to the phantom. A bulge detector was designed to detect a peak in the strain pattern along the phantom annulus. A bulge index was calculated using convolution of the annular strain with the bulge detector. The maximum annular bulge index was significantly different among patients with different degrees of paravalvular leakage. A higher bulge index was associated with higher degree of leakage. This novel method of quantification using 3D printed tissue-like models may aid in prospectively identifying patients at high risk for paravalvular leak (13), although further study is required.

A Flow Loop Used to Assess the Reproducibility of Hemodynamics in a 3D Printed Model
The flow loop was used to assess the reproducibility of hemodynamics in a 3D printed model of a patient with aortic stenosis. The flow loop consists of a mock ventricle, the compliance elements (C), resistance elements (R), a reservoir (Res), valves (V), and pressure and flow transducers (P and Q, respectively). (A and B) Patients’ 2D echocardiographic (Echo) image of the aortic root and corresponding images of the 3D printed model. (C and D) The Doppler velocity profile of the patient’s aortic valve and the 3D printed valve are shown. Echo = echocardiography.

Transesophageal Images
(A) Transesophageal images are shown, with the prosthesis deployment depth designated by the distance between the annulus and the ventricular end of the prosthesis (red lines). (B) The 3D printed phantom with radiopaque beads, which served as landmarks. (C) The 3D printed phantom with implanted prosthesis and 3D reconstructions of the CT scan of the phantom with (D) and without (E) the prosthesis. The strain distribution of the aortic root (F) and annulus (G) are shown. Reprinted with permission from Qian et al. (13). L = left coronary cusp; LVOT = left ventricular outflow tract; N = noncoronary cusp; R = right coronary cusp; TAVR = transcatheter aortic valve replacement.
Right-sided heart failure
Transcatheter caval valve placement has been suggested to treat patients with severe tricuspid valve regurgitation who are not candidates for surgical repair. This procedure has been shown in animal experiments to reduce valvular insufficiency and improve hemodynamics (14). Multimodality imaging including 3D printing was used by O’Neill et al. (15) to implant a SAPIEN XT valve (Edwards Lifesciences Corp., Irvine, California) at the right atrium–inferior vena cava junction in a patient with severe tricuspid regurgitation and decreased right ventricular systolic function. The patient was status post-mitral ring placement for mitral regurgitation and had undergone radiation therapy for treatment of lymphoma. She had developed significant abdominal ascites. Based on the 3D printed models created from CCT, the decision was made to use the SAPIEN 29XT valve as opposed to the SAPIEN 26T valve, which demonstrated gaps between the inferior vena cava and valve frame concerning for sites of possible paravalvular leakage. The patient was discharged after 1 week without recurrence of ascites at 4 months' follow-up (15). 3D printed models of the tricuspid valve have also been created from 3D echocardiographic datasets (16). Although these models lack the detail of the subvalvular apparatus, future work in this area could help in planning interventions for patients with significant tricuspid regurgitation.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy characteristically involves development of thick myocardium, most often of the left ventricle. Depending on the level of symptomatology of the patient, a septal myomectomy may be considered to relieve left ventricular outflow tract obstruction. 3D printing of the left ventricle (LV) to better outline the LV geometry has been described by a number of groups (17). Yang et al. (18) used this method to print the LV with detailed color coding of the papillary muscles in a 33-year-old female with syncope and dyspnea secondary to hypertrophic cardiomyopathy. The patient had asymmetrical thickening of the LV myocardium, predominantly involving the ventricular septum. A CCT dataset was used to create the virtual model, which was then printed on an Objet 500 Connex 3 (Stratasys). The model was constructed so that the surgeon was able to disassemble the various anatomic components. The patient did well after the myomectomy with significant decrease in the gradient across the left ventricular outflow tract (18).
Heart transplantation
A 3D printed heart and liver of a patient with complex CHD and for whom Fontan physiology failed has been used to plan heart and lung transplantation. The patient's anomalies consisted of situs inversus totalis, tricuspid atresia, pulmonary atresia, and a complex Fontan palliation (Figure 5). The 3D printed model provided improved understanding of potential surgical anastomoses prior to en bloc heart and liver transplantation from a donor with normally oriented thoracic and abdominal organs. The model provided valuable spatial information regarding the anatomy as a whole, including the abnormal orientation of the cardiac apex in the right chest and the complex Fontan connection (19).

3D Printed Heart and Liver of a 31-Year-Old Patient With Situs Inversus Totalis
(A) 3D printed heart and liver of a 31-year-old patient with situs inversus totalis, tricuspid atresia, pulmonary atresia, and complex Fontan palliation, shown for improved understanding of potential surgical anastomoses relationships prior to en bloc heart and liver transplantation. The coronal CT scan image (A), 3D virtual model (B), and 3D printed model (C) are shown. Reprinted with permission from Bramlet et al. (19). CS = coronary sinus; SVC = superior vena cava; other abbreviations are as in Figure 1.
Ventricular assist device placement
Ventricular assist device (VAD) placement can be challenging in patients who are atypical in terms of their size or have congenital cardiac malformations that render routine methods of placement obsolete. In patients with smaller chest cavities, 3D printing, or rapid prototyping, has been used to plan VAD placement (20). 3D modeling and virtual fitting was conducted by Karimov et al. (20) to allow verification of human implant-specific characteristics of the Cleveland Clinic continuous-flow total artificial heart device, such as outflow design and length, proper angles, and device orientation.
Up to one-fourth of patients with CHD will progress to HF by age 30 (21). Those patients with complex CHD are at highest risk for developing HF. This includes patients with a systemic right ventricle, which is inappropriately responsible for pumping to the systemic circulation when it normally supports low-pressure pulmonary circulation (22). Patients with single ventricle physiology, in which 1 of the ventricles is nonfunctional, are also at high risk for HF. These patients receive surgical palliation with a 3-stage Fontan procedure. Fontan palliation results in passive flow of deoxygenated blood from the systemic veins directly to the pulmonary arteries through a conduit while the single functional ventricle pumps oxygenated blood to the body (23).
Use of VADs to augment the cardiac output in patients with CHD and HF remains rare due in part to the highly variable anatomy and complex physiology in this population. Factors such as complex congenital malformations, heavy trabeculations, or a severely dilated ventricle can distort the usual anatomic landmarks used to identify the best position for cannula placement. 3D printed cardiac models of such patients with complex CHD can provide a physical guide to specific anatomic features that can make VAD and cannula placement challenging. The present authors previously published descriptions of the typical lesions in which 3D printed models would be most useful for VAD placement (24).
Figure 6 depicts a 3D printed model from CMR of the right-sided cardiac anatomy in a patient with severe Ebstein anomaly. There is displacement of the tricuspid valve into the right ventricular outflow tract with potentially severe tricuspid regurgitation. Distortion of the severely dilated right ventricle can be easily appreciated from the 3D model externally, and the displaced valve leaflets are seen internally. Given the marked alteration of the right ventricular architecture secondary to severe volume overload, a 3D model would be valuable in planning VAD inflow and outflow cannula placement.

3D Virtual Model and Corresponding Printed Model
3D virtual model (A and B) and corresponding printed model (C) of a patient with Ebstein anomaly. The RV is cropped to allow viewing of the intracardiac anatomy including the TV, which is apically displaced. MPA = main pulmonary artery; RA = right atrium; RV = right ventricle; TV = tricuspid valve.
Miller et al. (25) demonstrated the use of a 3D printed cardiac model to plan implantation of a Heartware VAD (Heartware International, Framingham, Massachusetts) in a patient with d-transposition of the great arteries after an atrial switch procedure and a systemic right ventricle. The model also incorporated the ribcage, to allow an assessment of device fit within the chest. Both rigid and flexible materials were used to create the cardiac models, and a suitable position for the inflow cannula was determined based on the position of the tricuspid valve annulus and trabeculations (25).
Uses for a Digital Model
Creation of a 3D printed cardiac model continues to be a relatively time- and labor-intensive process. This has led some to consider the alternative of using the source digital cardiac model for pre-procedural planning. Use of the virtual model has some considerable advantages including model material and time saved. Virtual models can also be cropped along different planes, whereas the cropping plane in a physical model, once printed, is no longer adjustable. Digital models allow the possibility of virtual interaction between 2 separate 3D reconstructions. For example, most relevant for heart failure patients, VAD implantation can be tested virtually. In patients with more complex cardiac spatial relationships (e.g., CHD), the ability to make subtle adjustments in device positioning with a digital model of the abnormal heart offers valuable insight. In d-transposition of the great arteries, for example, the aorta arises from the right ventricle and the pulmonary artery from the left ventricle. The Mustard and Senning procedures, in which there is rerouting of deoxygenated blood from the right atrium to the left side of the heart and of oxygenated blood from the left atrium to the right side of the heart using surgical baffling, were the treatments previously used for this lesion. Figure 7A illustrates a 3D model of a pulmonary venous baffle, from the left atrium, to the right atrium and systemic right ventricle in a patient who had undergone a Mustard procedure. In order to demonstrate possible VAD positioning, a Heartmate 2 (Thoratec, Pleasanton, California) was also segmented and virtually implanted into the systemic right ventricle. The anterior right ventricle was cropped to demonstrate the parallel relationship of the inflow cannula to the tricuspid valve inflow (Figure 7B). If desired, this virtual model can then be used to create a physical model on any 3D printer. Other investigators have published reports of virtual implantation of the total artificial heart and pediatric-specific VADs in children with heart failure (26,27). In the case of the total artificial heart, the device was implanted into a digital model of the entire thorax due to concern that the patient’s size was just at the acceptable lower limit for device implantation.

3D Model of the PVB in a Patient With d-TGA
(A) 3D model of the PVB in a patient with d-TGA after an atrial switch procedure, using an HM virtual implant. The inflow cannula is placed in the RV apex, and the outflow cannula in the AO. (B) The anterior aspect of the RV is cropped to show optimal inflow cannula position parallel to the direction of the TVI. AO = aorta; d-TGA = d-transposition of the great arteries; HM = Heartmate 2; PVB = pulmonary venous baffle; TVI = tricuspid valve inflow; other abbreviations are as in Figures 1 and 6.
Bioprinting
3D printing technology has found applicability in the fields of tissue engineering and regenerative medicine in the form of bioprinting. Bioprinting involves the process of laying down cells in a predefined spatial arrangement with or without use of a biocompatible scaffold, using 3D printing technology. In order to result in functional tissue, the cells must maintain their viability and specific cell function within their new environment. The potential applications for treatment of patients with HF are numerous and wide ranging. Wang et al. (28) reported using a 3D bioprinting strategy to create functional cardiac tissue capable of synchronized contraction, a characteristic of native myocardium. In patients with degenerative valve disease, the work of Duan et al. (29) holds promise in demonstrating the creation of living alginate/gelatin hydrogel aortic valve conduits, using 3D bioprinting. The authors successfully bioprinted the conduits with direct encapsulation of smooth muscle cells in the valve root and valve leaflet interstitial cells in the leaflets (29). Patient-specific coronary artery bypass grafts and the use of a bioprinted patch for repair of infarcted myocardium are additional areas of research that, at one time, might have seemed like theoretical futuristic concepts but are closer to becoming reality due to the immense work being done in this area (30,31).
Future Directions
In an era in which “precision medicine” and “personalized medicine” have become synonymous with high-quality patient care, we must strive to offer optimized treatment options that cater to the unique characteristics of the individual patient. 3D printing technology, whether in the form of cardiac models demonstrating complex CHD or a patch of bioprinted cells that can aid in healing infarcted myocardium, offers great potential to help us do just that. Although there are no definitive data yet available to show that 3D printed models improve outcomes in patients with CHD, 3D printed models have been shown to change the surgical approach used (32). A number of multicenter studies are ongoing to try to establish improvement in clinical outcomes. Such multicenter prospective studies are one of the primary means by which the roles of these planning tools can be reliably established and accepted. In addition, to increase use of this technology among those caring for patients with heart failure, a multidisciplinary approach is essential. Communication between the heart failure specialists, surgeons, and imaging team allows clear delineation of what additional anatomic information the 3D printed model can provide and the best method by which this can be accomplished. Although a one-size-fits-all mentality may have been acceptable in the past because of necessity or lack of options that allowed a better approach, it appears that 3D printing will continue to be a driving force, allowing us to more readily practice individualized medicine and offer the best quality of care for patients with HF.
1. : "2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America". J Am Coll Cardiol 2017; 70: 776.
2. : "Three-dimensional printing of models for surgical planning in patients with primary cardiac tumors". J Thorac Cardiovasc Surg 2013; 145: 1407.
3. : "Surgical planning, three-dimensional model surgery and preshaped implants in treatment of bilateral craniomaxillofacial post-traumatic deformities". J Oral Maxillofac Surg 2014; 72: 1138 e1.
4. : "Use of a three dimensional printed cardiac model to assess suitability for biventricular repair". World J Pediatr Congenit Heart Surg 2016; 7: 414.
5. : "Use of 3-dimensional printing to demonstrate complex intracardiac relationships in double-outlet right ventricle for surgical planning". Circ Cardiovasc Imaging 2015; 8. :e003043.
6. : "A novel approach to neonatal management of tetralogy of Fallot, with pulmonary atresia, and multiple aortopulmonary collaterals". J Am Coll Cardiol Img 2015; 8: 103.
7. : "Feasibility and validity of printing 3d heart models from rotational angiography". Pediatr Cardiol 2018; 39: 653.
8. : "3D slicer as an image computing platform for the quantitative imaging network". Magn Reson Imaging 2012; 30: 1323.
9. : "3D Printing of Medical Devices". Available at: https://www.fda.gov/medicaldevices/productsandmedicalprocedures/3dprintingofmedicaldevices/default.htm. Accessed August 31, 2018.
10. : "Replicating patient-specific severe aortic valve stenosis with functional 3D modeling". Circ Cardiovasc Imaging 2015; 8: e003626.
11. : "Two-year outcomes after transcatheter or surgical aortic-valve replacement". N Engl J Med 2012; 366: 1686.
12. : "3D printing based on cardiac CT assists anatomic visualization prior to transcatheter aortic valve replacement". J Cardiovasc Comput Tomogr 2016; 10: 28.
13. : "Quantitative prediction of paravalvular leak in transcatheter aortic valve replacement based on tissue-mimicking 3D printing". J Am Coll Cardiol Img 2017; 10: 719.
14. : "Percutaneous caval stent valve implantation: investigation of an interventional approach for treatment of tricuspid regurgitation". Eur Heart J 2010; 31: 1274.
15. : "Transcatheter caval valve implantation using multimodality imaging: roles of TEE, CT, and 3D printing". J Am Coll Cardiol Img 2015; 8: 221.
16. : "3D printing of normal and pathologic tricuspid valves from transthoracic 3D echocardiography data sets". Eur Heart J Cardiovasc Imaging 2017; 18: 802.
17. : "Scan, plan, print, practice, perform: Development and use of a patient-specific 3-dimensional printed model in adult cardiac surgery". J Thorac Cardiovasc Surg 2017; 153: 132.
18. : "Myocardial 3-dimensional printing for septal myectomy guidance in a patient with obstructive hypertrophic cardiomyopathy". Circulation 2015; 132: 300.
19. : "Impact of three-dimensional printing on the study and treatment of congenital heart disease". Circ Res 2017; 120: 904.
20. : "Human fitting studies of Cleveland Clinic continuous-flow total artificial heart". ASAIO J 2015; 61: 424.
21. : "Incidence and risk distribution of heart failure in adolescents and adults with congenital heart disease after cardiac surgery". Am J Cardiol 2006; 97: 1238.
22. : "Systemic right ventricle in adults with congenital heart disease: anatomic and phenotypic spectrum and current approach to management". Circulation 2018; 137: 508.
23. : "Surgical repair of tricuspid atresia". Thorax 1971; 26: 240.
24. : "3D printing to guide ventricular assist device placement in adults with congenital heart disease and heart failure". J Am Coll Cardiol HF 2016; 4: 301.
25. : "3D printing for preoperative planning and surgical simulation of VAD implantation in a failing right systemic ventricle". J Am Coll Cardiol 2018; 71: A545.
26. : "The Cleveland Clinic PediPump: virtual fitting studies in children using three-dimensional reconstructions of cardiac computed tomography scans". ASAIO J 2008; 54: 133.
27. : "Total artificial heart in the pediatric patient with biventricular heart failure". Perfusion 2014; 29: 82.
28. : "3D bioprinted functional and contractile cardiac tissue constructs". Acta Biomater 2018; 70: 48.
29. : "3D bioprinting of heterogeneous aortic valve conduits with alginate/gelatin hydrogels". J Biomed Mater Res A 2013; 101: 1255.
30. : "UV-assisted 3D bioprinting of nanoreinforced hybrid cardiac patch for myocardial tissue engineering". Tissue Eng Part C Methods 2018; 24: 74.
31. : "Human microvasculature fabrication using thermal inkjet printing technology". Biomaterials 2009; 30: 6221.
32. : "Three-dimensional printed models for surgical planning of complex congenital heart defects: an international multicentre study". Eur J Cardiothorac Surg 2017; 52: 1139.
Abbreviations and Acronyms
| 3D | 3-dimensional |
| ABS | acrylonitrile butadiene styrene |
| CMR | cardiac magnetic resonance |
| CCT | cardiac computed tomography |
| CHD | congenital heart disease |
| FDM | fused deposition modeling |
| HF | heart failure |
| LV | left ventricle |
| PLA | poly-lactic acid |
| TAVR | transcatheter aortic valve replacement |
| VAD | ventricular assist device |
Footnotes
Dr. Lipson is a co-founder of and holds equity in 3DBio, Inc. Dr. Bacha is a scientific council member and consultant for Cormatrix. Dr. Einstein has received research grants from Canon Medical Systems and Roche Diagnostics; and is a consultant for GE Healthcare. Dr. Jorde is an uncompensated consultant for Abbott. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}